Billing & Payment solutions
Practice management
Tebra makes it easy to successfully manage your medical billing and get paid faster.

ALL-IN-ONE
Billing & Payments
Practice management is just part of our all-in-one solution
Practice management
Insurance eligibility
Insurance claim submission
Patient payments
Patient statements
Robotic process automation
Managed billing
Billing partner program
KPI and workflow dashboard
Eligibility checks and patient authorizations
Charge capture and encounter review
Rejection and denial management
Claim submissions
Electronic remittance advice (ERA)
Robotic process automation (RPA)
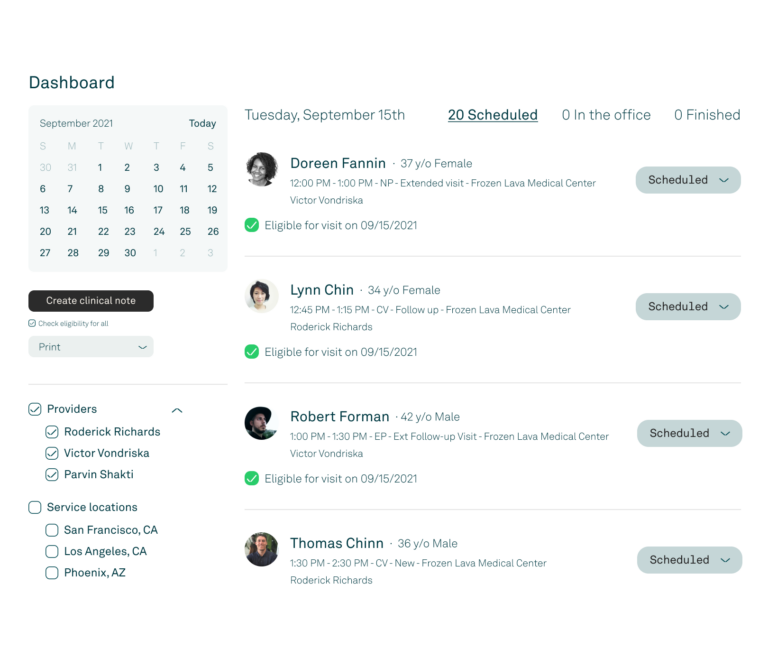
KPI and workflow dashboard
Save time and stay on track with our intuitive practice management dashboard. Easily review essential task lists, KPIs, and workflows.
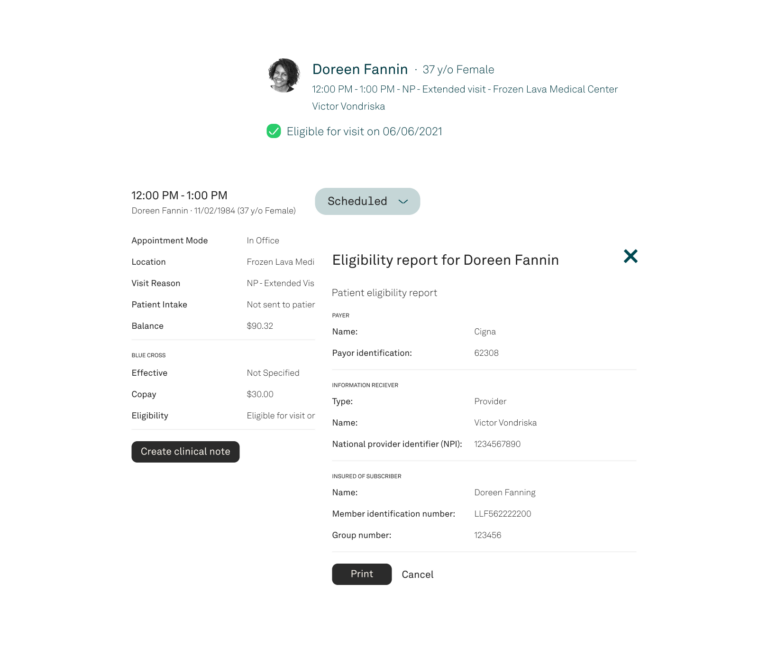
Eligibility checks and patient authorizations
Increase collections by verifying patient insurance ahead of time.
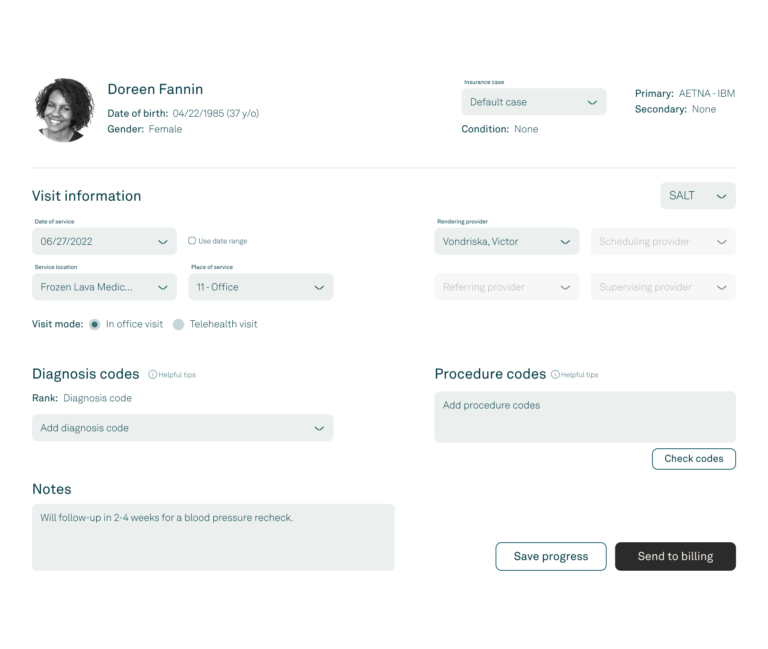
Charge capture and encounter review
View, enter, and improve claim accuracy to gain first-pass approvals.
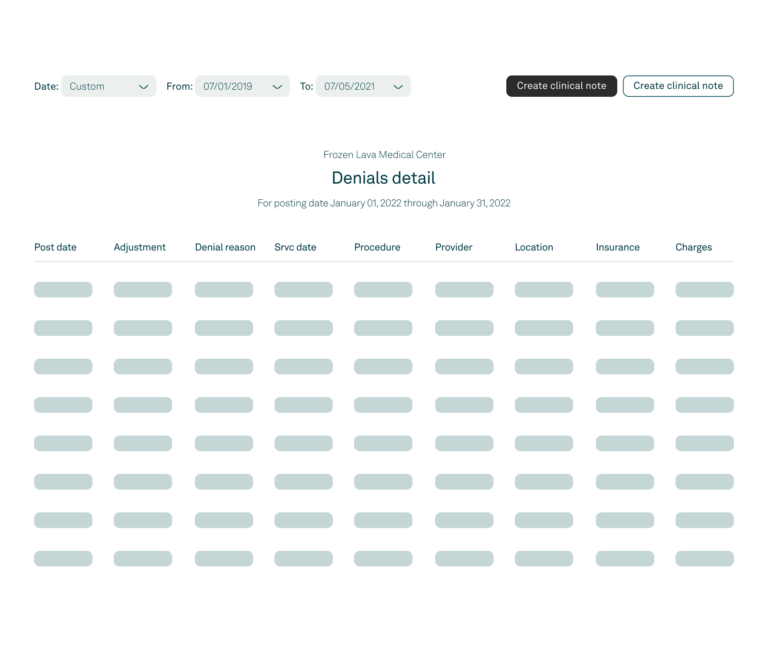
Rejection and denial management
Address the root cause of your denials to reduce the number you encounter on a daily basis.
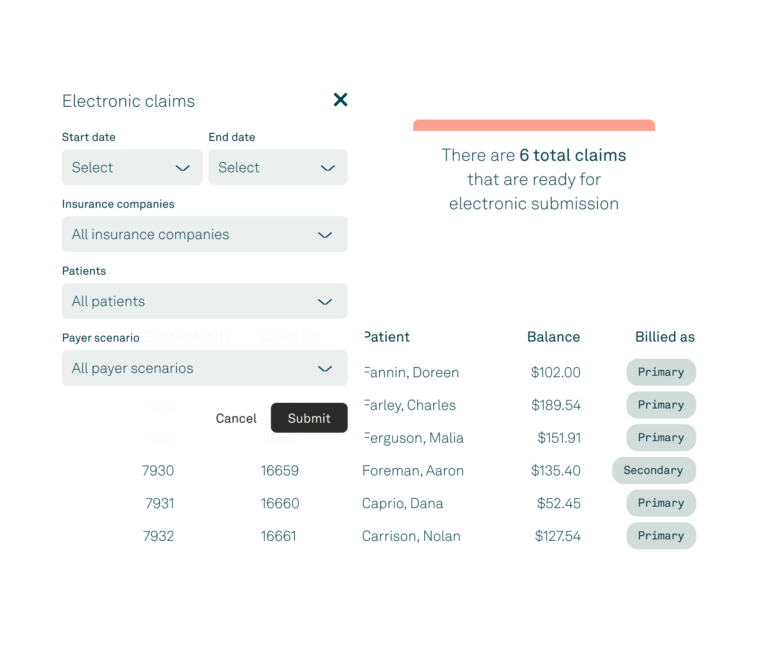
Claim submissions
Accurate electronic claim submissions can help you avoid costly delays and disruptions in cash flow.
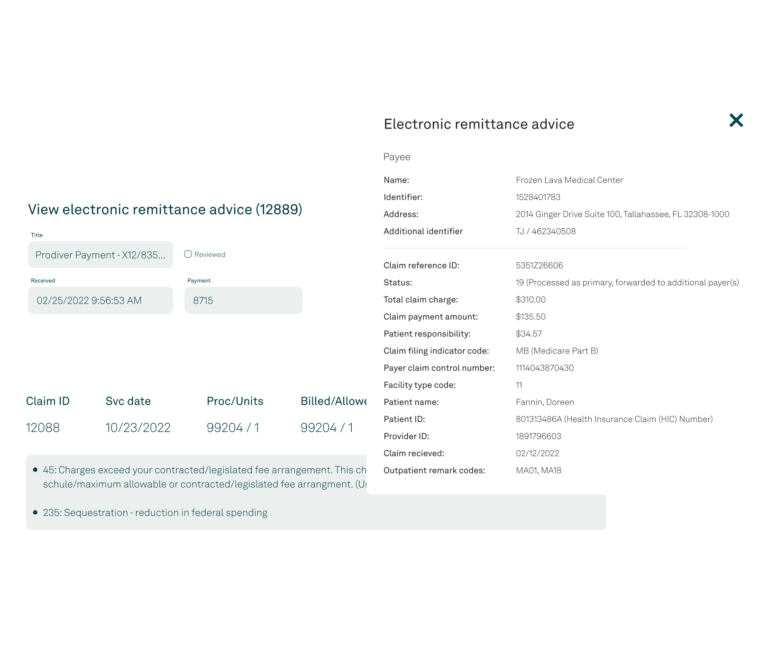
Electronic remittance advice (ERA)
Receive medical insurance payment explanations electronically to save time and drive speed to revenue.
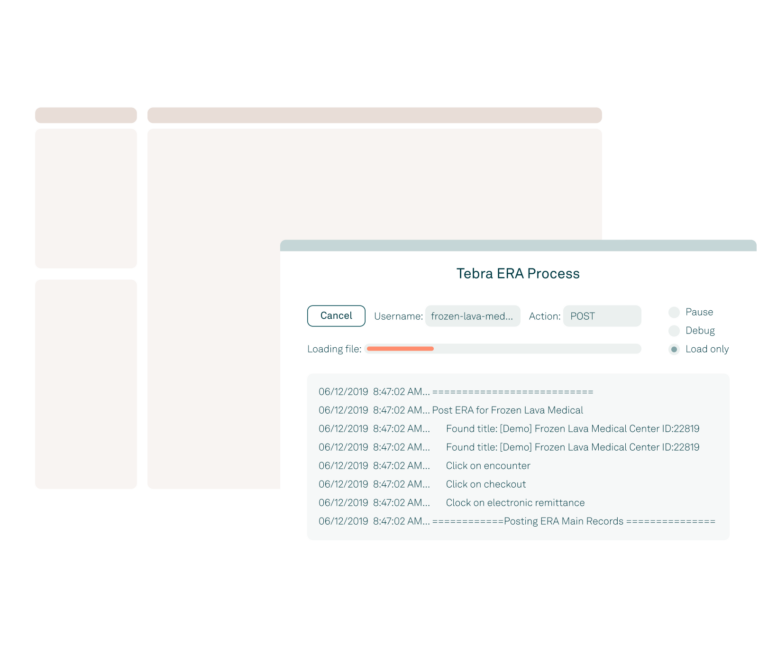
Robotic process automation (RPA)
Dramatically increase productivity and profitability with intelligent automation.
Resources
-
 Case study
Case studyHow a speech therapist went from house visits to opening 3 locations using Tebra
Chimezie Chidi founded Celebrations Speech Group to deliver 1-on-1 sessions to clients
Read more
-
 The Intake
The IntakeMedical insurance credentialing 101: Everything you need to know to avoid losing money and clients
From avoiding hours of paperwork to getting paid by insurance companies, find out what you need to know about medical insurance credentialing
Read article
-
 The Intake
The IntakeClean medical claims: What you need to know for increased revenue
It’s not enough to just be proficient at submitting clean claims. Get the latest trends in medical claims submission from a medical industry expert
Read article
